|
This is called anterior
because the cervical spine is reached through
the front of the neck. The approach is similar to a discectomy (anterior
approach), although a larger and more vertical incision in the neck
will often be used to allow more extensive exposure.
Laminotomy/Laminectomy
Laminectomy and laminotomy are open surgeries performed to relieve
pressure on the
spinal cord and/or spinal nerve roots by removing all or part of the
lamina. The lamina is
the thin part of the bones that make up the spine (vertebrae ), which
forms a protective
arch over the spinal cord.
A laminotomy removes a part of the lamina to make a larger opening
to relieve
pressure; a laminectomy removes all of the lamina on select
vertebrae and may also
remove thickened ligament tissue. They are typically performed under
general
anesthesia. Different terms are used to describe the laminectomy or
laminotomy
depending on where in the body they are performed. For example, in
the neck, the
term used is cervical laminectomy or laminotomy.
The choice of procedure depends on the location and severity of the
spinal problem that
requires treatment. Reducing pressure on the nerve roots often can relieve
leg or arm
pain and allow resumption of normal daily activities. Laminectomies and
laminotomies
are often performed in the course of a number of operations on the spinal
canal,
such as removal of a ruptured disc.
Lumbar Laminectomy
A lumbar laminectomy is used to relieve pressure on the lumbar
spinal cord or spinal nerve by widening the spinal canal. A small
section of the bony roof of the spine, the lamina, is removed to
create more space for the nerves. A surgeon may perform a lumbar
laminectomy with or without fusing vertebrae or removing part of a
disc. It is also known as open decompression.
Posterior Cervical Laminectomy
This surgical procedure is used to remove the pressure on the spinal
cord by opening the spinal canal from the back of the cervical spine
to make the spinal canal larger.
Medial Facetectomy
Facetectomy is an invasive surgical procedure that is performed to
relieve pressure on spinal nerves. The procedure involves exposing
the affected vertebra and removing one or both of the articulating
facet joints that are rubbing against the nerve. Sometimes a
laminotomy is performed in conjunction with a facetectomy. Most
patients are given a general anesthetic for the procedure.
Foraminotomy
Foraminotomy is an operation that widens or enlarges the opening or
foramen where a nerve root exits the spinal canal. Bulging,
herniated discs or joints thickened with age can cause narrowing of
the space through which the spinal nerve exits and can press on the
nerve, resulting in pain, numbness, and weakness in an arm or leg.
Small pieces of bone over the nerve are removed through a small
slit, allowing the surgeon to cut away the blockage and relieve the
pressure on the nerve. This may performed on any level of the spine,
and most patients undergo the procedure with general anesthesia.
Spine fusion
Spinal fusion is an invasive surgical procedure used to strengthen
the spine, treat spinal instability, and prevent painful movements.
Spinal fusion is usually performed at the end of other surgical
procedures for the spine, such as discectomy, laminectomy, and
foraminectomy.
The spinal discs between two or more vertebrae are removed and the
adjacent vertebrae are “fused” together by bone grafts and/or metal
devices secured by screws. The patient's bones will grow over the
graft. Spinal fusion may result in some loss of flexibility in the
spine and requires a long recovery period to allow the bone grafts
to grow and fuse the vertebrae together.
Spinal disc replacement
Spinal disc replacement surgery is also called as “total disc
replacement, inter vertebral disc arthroplasty or, artificial disc
replacement”. In this procedure, intervertebral degenerated discs in
the spine are replaced with artificial (plastic or metal) discs in
the upper or lower spine. This procedure is used to treat severe,
chronic lumbar pain and cervical pain that resulted from
degenerative disc disorder. It allows more motion in the spine than
some spine fusion surgeries, and may prevent the breaking down of
premature adjacent spine levels. Not everyone is eligible for this
procedure.
Minimally Invasive Spine Surgery
Dr. Berti is one of few neurosurgeons who specializes in
minimally-invasive spine surgery (MIS). Minimally-invasive
procedures take place through one or more short incisions, as
opposed to conventional, open surgery's deeper and longer cuts.
These smaller incisions lead to less post-operative pain, quicker
recovery, less blood loss, and shorter hospital stays.
Typically, in MIS, Dr. Berti inserts an endoscope through a small
incision into the area to be worked on. An endoscope is a long, thin
tube with a lighted camera on its tip. Dr. Berti can then monitor
the surgical site on a high-definition monitor. MIS requires
specially designed instruments, which are placed through the small
incisions made earlier. Not every patient is eligible for this
procedure.
Pain management (Epidural steroid injections, Facet Blocks)
Dr. Berti explores all possible conservative, non-surgical
procedures to treat back pain before recommending surgery. His goal
is to provide safe pain relief for his patients. He offers epidural
steroid injections and facet blocks among others. These injections
are used in conjunction with a thorough physical therapy plan. These
injections are temporary solutions, effective from one week up to
one year, that help the patient with acute episodes of pain or with
progressing in their rehabilitation program.
Steroid injections are used in the cervical (neck), thoracic
(mid-spine), and lumbar (lower back) regions, and can also treat
radicular pain such as sciatica. The steroidal injection delivers
medication directly or very near to the source of pain, while also
avoiding the side effects caused by oral steroids. Injecting these
steroids directly can noticeably decrease the inflammation
associated with spinal stenosis, hernias, and degenerative disc
disease, and is thought to also flush out inflammatory proteins. The
most commonly performed injection is an epidural steroid injection.
Facet joints are two hinge-like joints of the spine that link
vertebrae together. They are located on the back of the spine. A
facet block or facet joint injection is a surgical procedure that
involves injecting a time-release steroid medication into the facet
joint to reduce inflammation, under imaging guidance. The facet
block is designed to relieve pain so that a patient can tolerate
physical therapy, and to diagnose the cause and location of the back
pain.
Vertebroplasty and Kyphoplasty
Vertebroplasty is one of the minimally-invasive procedures Dr. Berti
uses to strengthen and stabilize a spinal fracture, and relieve pain
caused by that fracture. The procedure is performed with the patient
sedated (either under general anesthesia or a local anesthetic with
intravenous sedation). The doctor will inject a specially formulated
acrylic bone cement into the diseased vertebra under x-ray guidance.
Vertebroplasty generally takes about one hour to perform per
vertebra.
Kyphoplasty is a newer, minimally-invasive procedure performed on
patients with compression fractures of the spine. The procedure is
similar to vertebroplasty, but adds one step before the cement is
injected into the vertebra. The patient is anesthetized, the bone is
drilled, and one balloon (called a bone tamp) is inserted into each
side of the vertebra. The two balloons are inflated with a contrast
medium and expanded until the desired height is reached, and then
removed. The spaces created by the balloons are filled with cement.
This procedure can restore height to the spine and can reverse
deformity of the spine. It works best on recent compression
fractures.
Ventriculoperitoneal shunt
A ventriculoperitoneal shunt is a surgery performed to relieve
increased inctracranial pressure caused by hydrocephalus. A shunt
system consists of the shunt, a catheter, and a valve. One end of
the catheter is placed within a ventricle inside the brain, or in
the CSF outside the spinal cord. The other end is usually placed
within the peritoneal cavity, or wherever the physician decides to
place it for CSF reabsorption. A shunt is a flexible and sturdy
plastic tube.The valve is located along the catheter and should
regulate and maintain a one-way CSF flow. This procedure is
performed in an operating room under general anesthesia.
Craniotomy:
A craniotomy is a cut that opens the skull (cranium). This surgical
procedure is used by neurosurgeons for a variety of neurological
conditions and diseases, including brain tumors, arteriovenous
malformations, swelling of the brain, and skull fractures, and is
often a first step in other complex procedures. A craniotomy is
performed under general anesthesia.
Stereotactic biopsy:
Stereotactic biopsy is a minimally-invasive procedure used to remove
a small amount of tissue from a tumor site. The tissue will be
examined by a pathologist under a microscope to diagnose the tumor.
A stereotactic biopsy is performed for deeper tumors in critical
locations with the use of a titanium stereotactic headframe and a
computer, which are used to create a reference for all imaging and
scants to a coordinate system, allowing for a precise approach. The
procedure generally takes around 1 1/2 hours.
Microsurgery:
In microsurgery, surgeons view the minute structures within the body
they operate on through a compound operating microscope.
Neurosurgeons can operate on delicate nerves, treat vascular
abnormalities, and tumors precisely with miniaturized instruments.
Stereotactic Radiosurgery (Gamma Knife, Cyberknife, LINAC)
Stereotactic radiosurgery (SRS) is an alternative to open-skull
brain surgery, spine surgery or microsurgery, offering significantly
fewer complications and lower risk than open surgery. It is an
advanced form of radiation therapy, focusing high-powered x-rays or
gamma rays onto a small area in contrast to traditional radiation
therapy's approach.
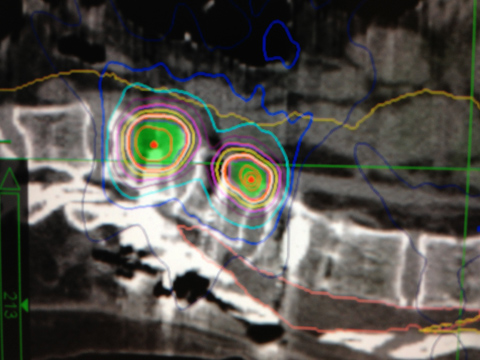
Stereotactic radiosurgery uses sophisticated 3-D computerized
imaging to precisely target and deliver narrow, highly concentrated
doses of radiation to the affected tissue. It is most commonly used
in the treatment of brain or spinal tumors and brain metastases from
other cancer types, and is generally restricted treating only small
tumors with well-defined edges. It is not considered a surgical
procedure because there is no incision involved, and no general
anesthesia is required.
Radiation therapy requires a multi-disciplinary approach. The team
of treatment specialists may include a radiation oncologist, a
neurosurgeon, a medical radiation physicist, a dosimetrist, a
radiation therapist or radiation therapy nurse, and a neuro-oncologist,
among others. As your neurosurgeon, Dr. Berti will oversee the
treatment process and interpret the results of the procedure with
the radiation oncologist.
There are many types of radiation therapy. Dr. Berti specializes in
Gamma Knife and CyberKnife.
Gamma Knife:
Gamma Knife is a stereotactic radiosurgical treatment that safely
delivers a single, large dose of gamma radiation to the targeted
brain tumor or affected tissues in the brain with precision. The
radiation kills the cancer cells at a molecular level by disrupting
its DNA, thus interfering with the tumor's ability to survive.
Gamma Knife requires the use of a stereotactic, 3-D reference frame
which is attached to the patient's head. This frame provides a
reference which can be seen on the imaging equipment, which can
provide exact coordinates for the target. This frame keeps the
patient's skull perfectly still for further accuracy.
Approximately 201 sources of Cobalt-60are available in the Gamma
Knife treatment unit. Thousands of radiation beams can be generated
from the sources with a level of accuracy of more than 0.5 mm, or
the thickness of one strand of hair. An individual radiation beam is
too weak to damage tissue on its path to the target. The accurate
intersecting of all the beams on the target results in radiation
sufficient to treat the targeted area. A full dose of radiation can
be delivered during a single session. Lesions from 5 to 40 mm can be
treated. This is an outpatient procedure that takes roughly 30
minutes.
CyberKnife:
The CyberKnife Robotic Radiosurgery system is a safe, non-invasive
treatment alternative to conventional surgery for both benign and
malignant tumors throughout the whole body, including the spine and
brain. There is no incision, no blood, and it, too, is an outpatient
procedure. The treatment accurately delivers high doses of radiation
to tumors. The radiation kills the cancer cells at a molecular level
by disrupting its DNA, thus interfering with the tumor's ability to
survive. The precisely targeted beams destroy tumors painlessly,
without incisions, and spare the surrounding healthy tissue.
The CyberKnife uses a compact, lightweight linear accelarator (LINAC)
mounted on a robotic arm to deliver as many as 1,400 highly
pinpointed beams of radiation to control or destroy the tumor in
conjunction with a sophisticated Synchrony Respiratory Tracking
System to monitor the movement of the tumor and the patient's
breathing pattern, helping the surgeon maintain tighter control in
real time and sparing even more healthy tissue. This procedure
should last from 30 to 90 minutes. The patient may need to come back
if the treatment is being delivered in stages.
Microvascular decompression
Microvascular decompression (MVD) is a surgical procedure Dr. Berti
employs to relieve abnormal compressions of cranial nerves for some
patients with trigeminal neuralgia when medication to provide relief
to patients does not work or causes serious side effects. MVD is
performed to relieve symptoms caused by the compression of a nerve
by an artery or a vein. When performing an MVD, your doctor will
perform a craniotomy, and insert a tiny surgical sponge between the
compressing blood vessel and the nerve, isolating the trigeminal
nerve from the pulsating effect and pressure of the blood vessel. It
requires general anesthesia.
Percutaneous stereotactic rhizotomy
Percutaneous steretotactic rhizotomy (PSR) is an alternative,
minimally-invasive outpatient procedure performed to relieve the
pain caused by trigeminal neuralgia, glossopharyngeal neuralgia, and
cluster headaches. PSR involves the surgeon passing an electrode
inducer (hollow needle), into the selected nerve at the base of the
skull. A heating current passed through the electrode destroys a
portion of the nerve fibers- not the entire nerve- alleviating the
pain, but potentially resulting in facial numbness.
Percutaneous glycerol rhizotomy
Percutaneous glycerol rhizotomy is a procedure performed under local
anesthesia. The doctor will insert a needle through your cheek into
a natural opening at the base of your skull (foramen ovale). The
needle will be maneuvered to the space surrounding the trigeminal
ganglion, where the trigeminal nerve divides into three branches,
and part of its root. Images are taken to confirm the proper
placement of the needle, and then the sterile chemical glycerol is
injected. This injures the nerve mildly, with minimal risk of
permanent damage or facial paralysis. This treatment will produce
relief for a majority of patients, but some may have a recurrence of
pain later on.
Percutaneous balloon compression
Another option for pain control, the percutaneous balloon
compression procedure is performed while the patient is under
general anesthesia. A needle is inserted into a small opening at the
base of the skull. This needle is threaded with a special small
catheter with an inflatable balloon attached at the end. The balloon
is inflated with enough pressure to compress and injure the
trigeminal nerve root.
Balloon compression is a successful treatment for most people, and
lasts for some time. Some patients experience facial numbness. Many
patients develop weakness in the chewing muscles, at least
temporarily.
Motor cortex stimulation
Dr. Berti may suggest using motor cortex stimulation (MCS) to
trigeminal neuralgia for a select group of patients. The patient
selection process includes a number of factors, assessing
cardiovascular risk, the patient's likelihood of positive outcomes
with the surgery, previous treatments, and mental health, among
others.
MCS requires implanting electrodes over the primary motor cortex.
One or more electrodes are placed outside the dura (the outermost
layer of the meninges surrounding the brain and the spinal cord)
over the motor cortex via a small craniotomy or burr hole. These
electrodes are connected to an implanted, battery-powered
neurostimulator. The patient adjusts the electrical impulses with an
external radio transmitter to alleviate pain.
|