|
made. A frame is attached
to the patient's head, a scan is obtained, and then the patient is
taken to the operating area where a small hole is drilled in the
skull to allow access to the abnormal area. A small sample of
the tissue is obtained for examination under the microscope.
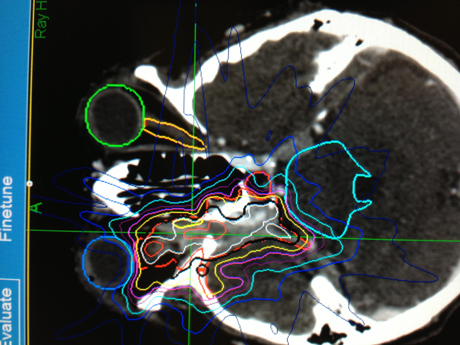
Stereotactic Radiosurgery
(such as Gamma Knife and Cyberknife) is a technique that focuses the
radiation with many different beams on the target tissue. This
treatment tends to incur less damage to tissues adjacent to the
tumor. Currently, there is no data to suggest one delivery system is
superior to another in terms of clinical outcome, and each has its
advantages and disadvantages. (link to appropriate procedure on
procedures page)
Stereotactic
Radiosurgery (such as Gamma Knife and Cyberknife) is a technique
that focuses the radiation with many different beams on the target
tissue. This treatment tends to incur less damage to tissues
adjacent to the tumor. Currently, there is no data to suggest one
delivery system is superior to another in terms of clinical outcome,
and each has its advantages and disadvantages.
The following are types of brain tumors Dr. Berti operates:
Chordomas: A chordoma is a rare malignant tumor that arises from
notochord remnants. Chordomas account for 1 to 4% of all bone
tumors. They occur in older adults, usually between fifty and
seventy years old.
Symptoms: The symptoms depend on the location of the tumor. For
example, sacrococcygeal tumors present as lower back pain, or tumors
in the cervical spine can present as pain at the base of the skull.
The bone surrounding the tumor is gradually and completely
destroyed.
Treatment: Treatment of chordomas can be difficult due to the
location of the tumor. Complete resection of the tumor and
subsequent radiation therapy are recommended.
Surgery (link to appropriate procedure on procedures page)
Stereotactic Radiosurgery (link to appropriate procedure on
procedures page)
Craniopharyngiomas: Craniopharyngiomas are benign brain tumors that
occur near the pituitary gland and pituitary stalk. They are
typically both cystic and solid in structuere, and can occur early
in childhood and adolescence, or later in life. They're usually not
discovered until they compress nearby important structures. They are
benign tumors, but they tend to adhere to structures around the
pituitary gland and stalk, including the optic nerves, optic chiasm,
intracranial arteries, and the brain itself.
Symptoms: While not malignant, craniopharyngiomas can cause a
variety of problematic symptoms depending on their location. One of
these tumors can cause partial or complete pituitary hormone
deficiency if the tumor compresses the pituitary stalk or gland,
which may lead to stunted growth, delayed puberty, loss of normal
menstrual function or sexual desire, increased sensitivity to cold,
fatigue, constipation, dry skin, nausea, low blood pressure, and
depression.
The compression of the pituitary stalk can also cause diabetes
insipidus, a condition where the kidneys cannot conserve water, and
can increase prolactin levels, causing a milky discharge from the
breast (galactohhrea). A person can experience loss of vision if the
tumor compresses the optic chiasm or nerves. If the tumor encroaches
on the hypothalamus, an area at the base of the brain that controls
body temperature, hunger, and thirst, may result in obesity,
increased drowsiness and temperature regulation abnormalities.
Other, rarer symptoms may include personality changes, headache,
confusion, and vomiting.
Treatment:
Surgery
Stereotactic radiosurgery
Hormonal Replacement Therapy
Gangliocytomas: A gangliocytoma is related to a ganglioglioma.
However, it only contains neural ganglion cells. It is a rare,
benign (WHO grade I) tumor. Gangliocytoma may occur throughout the
central nervous system, but are most commonly found in the temporal
lobes. Symptoms may include increased intracranial pressure,
headache, and visual disturbance.
Treatment:
Surgical resection
Glomus jugulare: Glomus jugulare tumors may occur in the temporal
bone in the skull, in an area called the jugular foramen, or the
glomus bodies located within the ear. They are the most common
tumors of the middle ear, and can affect the ear, upper neck, base
of the skull, and the surrounding blood vessels and nerves. These
tumors are slow-growing and involve the surrounding blood vessels,
and are most common in women.
Symptoms: Symptoms include hearing loss with pulsing ringing in the
ear, dizziness, weakness or loss of movement in the face, ear pain
and difficulty swallowing. Physical exams will find hearing loss and
abnormalities of the cranial nerves that control swallowing,
gagging, shoulder shrugging and tongue movements. A red/blue pulsing
mass can often be seen upon examining the eardrum.
Treatment:
Glomus jugulare tumors are rarely cancerous and do not tend to
spread to other parts of the body. However, treatment may be needed
to relieve symptoms. The main treatment is surgery. Surgery is
complex and is usually done by both a neurosurgeon and a head and
neck surgeon (neurotologist). In some cases, a procedure called
embolization is performed before surgery to prevent the tumor from
bleeding too much during surgery. After surgery, radiation therapy
may be used to treat any part of the tumor that could not be removed
completely.
Surgery
Stereotactic Radiosurgery
Meningiomas: A meningioma is a tumor that grows from the meninges,
layers of tissue that cover your brain and spinal cord. Meningiomas
are graded from low to high; the lower the grade, the lower the risk
of recurrance and aggressive growth. The majority of meningioma
cases are noncancerous (benign), athough a meningioma can be
cancerous (malignant) in rare cases.
Meningiomas typically arise in adulthood and are more common in
women, but they can occur at any time. The causes of meningiomas
aren't clear, but a few predisposing factors, such as genetics,
trauma, and exposure to radiation (for example, the survivors of
Hiroshima have an increased incidence of these tumors).
Symptoms include changes in vision, such as seeing double or
blurriness, headaches that worsen with time, hearing loss, memory
loss, behavioral and cognitive changes, seizures, and weakness in
the arms or legs.
Treatment: Surgery is the standard treatment. If the surgeon cannot
completely remove the tumor, he or she may recommend radiation
therapy.
Stereotactic Radiosurgery
Pineocytomas: A pineocytoma, also known as a pinealocytoma or
pinealoma, is a rare, slowly-growing, benign tumor of the pineal
gland of the brain. This brain tumor arises from the cells of the
pineal itself. Since pinealocytoma is rare, other types of tumors
are more common in the pineal region, such as a pineal germinoma or
even a glioma. There is usually no known cause for pineal tumors.
Most pineocytomas are considered low-grade or benign tumors.
However, tumors of the pineal gland itself can very in
aggressiveness with high-grade or malignant variants also occurring.
These high-grade variants are termed pineoblastomas and display much
more primitive or undifferentiated pathology.
Symptoms: For this reason, as a pineal tumor, such as a pineocytoma,
enlarges it can compress the aqueduct and block the normal flow of
cerebrospinal fluid. This can lead to a condition known as
hydrocephalus which results in enlargement of the ventricles and
increased pressure in the head. This can lead to symptoms such as
headache, nausea, vomiting and finally neurological deterioration as
it becomes more severe.
Other symptoms which can occur in some patients include a paralysis
of upward gaze of the eyes (due to compression of part of the brain
stem called the superior colliculi), disturbances of gait and
precocious puberty in children.
Treatment:
Surgical Removal via craniotomy (link to appropriate procedure on
procedures page)
Chemotherapy
Gamma Ray Therapy
CyberKnife Therapy
Pituitary Adenomas: Pituitary adenomas are typically benign,
slow-growing tumors that arise from cells in the pituitary gland.
They rarely spread to other parts of the body. Pituitary adenomas
are relatively common in the population, occurring in 1 out of every
1000 people, typically in people in their 30s and 40s. Pituitary
tumors may be hormone-producing (functioning) or hormone-inactive
(non-functioning).
Symptoms:
Functional adenomas will generally present with symptoms related to
endocrine imbalance or dysfunction. For example, an overproduction
of growth hormone will result in giantism. Non-functioning adenomas
may present with symptoms related to the tumor encroaching on
surrounding structures. A growing adenoma can compress important
vascular and neurological brain structures. Some of these symptoms
include visual loss (from the adenoma encroaching on the optic
nerve), pituitary failure, headache, and pituitary apoplexy, a
surgical emergency.
Treatment:
Microsurgery
Surgical resection
Radiation Therapy (Gamma Knife, CyberKnife)
Medication Therapy
Schwannomas: These tumors arise from schwann cells which form a
protective sheath around the body's nerve fibers. Also known as
vestibular schwannomas, neurilemmoma, or acoustic neuromas, these
tumors may grow on one or both sides of the brain and are
potentially curable with surgery or stereotactic radiosurgery.
They're typically benign and surgically removed when possible. They
usually appear as a single tumor, only rarely developing into
multiple tumors.
One of the more common forms of this tumor affects the eighth
cranial nerve, which contains nerve cells important for balance and
hearing. Hearing loss on the side where the tumor grows is a common
symptom. Schwannomas can also appear on the roots of the nerves that
come off of the spinal cord. Symptoms depend on which nerve is
affected, and may include tinnitus or balance problems.
Treatment:
Surgical removal
Radiotherapy
Gliomas: The most common form of primary brain tumor is called a
glioma. They arise from glial (or non-neuronal) cells, which provide
support and protection for neurons. There are four types of gliomas:
astrocytomas, ependymomas, oligodendrogliomas and mixed gliomas.
Astrocytomas are the most common glioma and can occur in most parts
of the brain (and occasionally in the spinal cord). Types of
astrocytomas include pilocytic astrocytoma (grade 1), low-grade
astrocytoma (grade II), anaplastic astrocytoma (grade III), and
glioblastoma (grade IV). Glioblastoma multiforme is the most common
and aggressive astrocytoma, and typically penetrates the surrounding
area of the brain where it is located. This particular tumor affects
adults, and is more common in males.
Symptoms of some astrocytomas may include seizures or convulsions,
trouble speaking, headaches, difficulty thinking or speaking, loss
of vision or vision changes, nausea or vomiting, and others. Surgery
is the standard treatment, and may be used in combination with
chemotherapy and radiation therapy, depending on the grade of the
tumor.
Ependymomas begin in cells lining the brain ventricles which contain
cerebrospinal fluid (CSF), a fluid that protects the brain and
spinal cord. These tumors are rare and slow-growing, and can be
found anywhere in the brain or spine, although in adults its
location is typically spinal.
Symptoms of ependymomas in the brain vary depending on its location.
Some symptoms include seizures and raised intracranial pressure,
which will cause headaches, neck pain, vomiting, and irritability.
Surgical removal is typically recommended for low-grade brain and
spinal tumors. After surgery, any leftover tumor tissue in the brain
is usually treated with radiation therapy.
Oligodendrogliomas begin in cells called oligodendrocytes, which
support and nourish the cells that transmit nerve impulses.
Oligodendrogliomas are normally found in the main part of the brain
(cerebrum), and occur primarily in adults. Symptoms depend on where
the tumor is located, but seizures, visual loss, and motor weakness
are a few of the more common types. Treatment options include
surgery, radiation and chemotherapy.
Mixed gliomas have more than one type of tumor cell, including
astrocytes, ependymomas and oligodendrocytes. The most common site
for a mixed glioma is the cerebrum, and are more common in men than
women. Symptoms may include headache, speech or motor change, and
seizures. Treatment recommendations are based on which of the cell
types is most aggressive.
Treatment:
Treatment depends on the type of tumor being treated. Surgical
removal is typically recommended for most low-grade brain and spinal
tumors. After surgery, any left over tumor tissue in the brain is
usually treated with radiation therapy.
Surgery (link to appropriate procedure on procedures page)
Chemotherapy
Radiation therapy
Medulloblastomas: A brain tumor usually located in the cerebellum or
brain stem, this tumor can spread to the spinal cord through
cerebrospinal fluid. It may obstruct the fourth ventricle, causing
hydrocephalus. It is more common in children, but may occur in
adults.
Symptoms include headaches, lethargy, early morning vomiting, lack
of coordination, double vision, behavioral or personality changes,
and signs of pressure seen behind the eye when examined with an
ophthalmoscope.
Treatment:
Surgery
Chemotherapy
Radiation Therapy
Other types of brain tumors:
Hemangioblastomas are slow-growing, benign tumors located most
commonly in the cerebellum, but may be found in the spinal cord.
These tumors originate in the blood vessels, and often involve
cysts. They are found typically in males and females from the age of
40 to 60. Symptoms include balance problems, headaches, and nausea
and vomiting.
Treatment:
Surgery is the standard treatment.
Radiation therapy is used in inoperable lesions. (link to
appropriate procedure on procedures page)
Rhabdoid tumors are rare, highly aggressive tumors that spread
throughout the central nervous system, and often appear in several
sites in the body, especially the kidneys. They can be difficult to
classify, being mistaken with medulloblastomas. They are found
mostly in children, but can occur in adults. Symptoms depend on the
location of the tumor in the body, but may include balance problems.
An external tumor might cause noticeable lumps.
Treatment:
Surgery is performed to remove as much of the tumor as possible,
followed by chemotherapy and radiation therapy.
|